Offensive smells from wounds, ulcers, fistulas, and bodily fluids are often ignored in medical care. These odours affect mental well-being of patients and have social & economic consequences.
Understanding the pathophysiology of internal odour
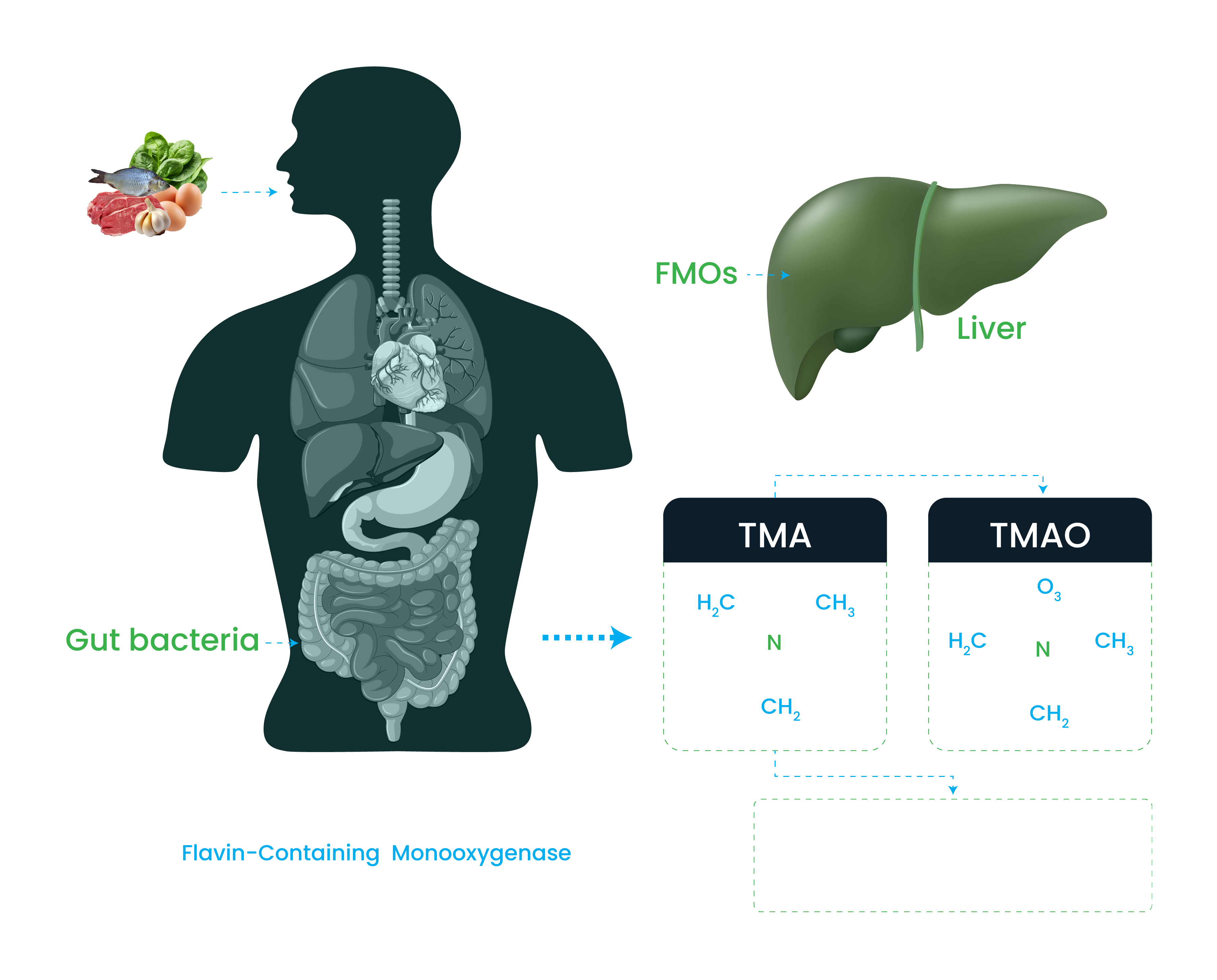
Trimethylaminuria is responsible for generation of odour in urine and faces.
- Accumulation of Trimethylamine (TMA) occurs mainly due to reduction in the conversion of Trimethylamine (TMA) to less odorous Trimethylamine-N-oxide (TMAO)
- This conversion is mediated via FMOs enzyme in the liver.
- FMOs enzyme activity is compromised due to mutations in the in FMOs genes.
- Non-functional or structurally altered enzyme impede Trimethylamine (TMA) conversion into Trimethylamine-N-oxide (TMAO), causing accumulation of Trimethylamine (TMA) and subsequent body odour.
 ODOUR
ISSUES IN OSTOMY
ODOUR
ISSUES IN OSTOMY
- Ostomies can cause significant distress for patients, with offensive odour affecting 59% of patients.
- Odour Control in ileostomy and colostomy surgery is crucial for patient comfort and quality of life.
- Odour in stoma is a chronic condition and requires due attention.
 ODOUR ISSUES
IN INCONTINENCE
ODOUR ISSUES
IN INCONTINENCE
- The fear of producing malodours that can be detected by others is a daily cause of anxiety for millions of people with incontinence.
- About one in three women experiencing incontinence are concerned about odour-related issues.
- Significantly large number of elderly suffer from incontinence and associated body odour and since it is a chronic condition it requires a solution which is safe and effective.